Difference between revisions of "IPLab:Lab 1:Lung Abscess"
(→Clinical Summary) |
(→Images) |
||
| (2 intermediate revisions by the same user not shown) | |||
| Line 2: | Line 2: | ||
This 67-year-old male with advanced colon cancer underwent palliative surgery to remove a bowel obstruction. During the surgery the patient had several episodes of hypotension and after surgery he required ventilator support. Four days later the patient developed a fever and his white blood cell count was 15,256 cells/mm3. A chest x-ray demonstrated infiltrates in both lungs, which worsened over the next several days. His overall condition continued to deteriorate and he died 12 days after surgery. | This 67-year-old male with advanced colon cancer underwent palliative surgery to remove a bowel obstruction. During the surgery the patient had several episodes of hypotension and after surgery he required ventilator support. Four days later the patient developed a fever and his white blood cell count was 15,256 cells/mm3. A chest x-ray demonstrated infiltrates in both lungs, which worsened over the next several days. His overall condition continued to deteriorate and he died 12 days after surgery. | ||
At autopsy, the lungs were markedly consolidated and had several focal abscesses that were 2 to 4 cm in diameter. Liquefied material poured out from these abscesses when the lungs were sliced. | At autopsy, the lungs were markedly consolidated and had several focal abscesses that were 2 to 4 cm in diameter. Liquefied material poured out from these abscesses when the lungs were sliced. | ||
| − | |||
| − | |||
| − | |||
== Images == | == Images == | ||
| Line 10: | Line 7: | ||
File:IPLab1LungAbscess1.jpg|This is a gross photograph of the lungs from this case. Note the abscesses (arrows) especially in the lower lobes. The entire lung is consolidated. | File:IPLab1LungAbscess1.jpg|This is a gross photograph of the lungs from this case. Note the abscesses (arrows) especially in the lower lobes. The entire lung is consolidated. | ||
File:IPLab1LungAbscess2.jpg|This is a closer view of the lung from this case. In this section of upper lobe there are multiple areas of early abscess formation (arrows). Note the circumscribed whitish-tan lesions. These lesions are filled with white blood cells. | File:IPLab1LungAbscess2.jpg|This is a closer view of the lung from this case. In this section of upper lobe there are multiple areas of early abscess formation (arrows). Note the circumscribed whitish-tan lesions. These lesions are filled with white blood cells. | ||
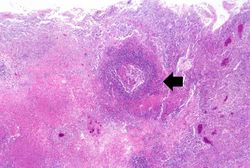
| − | File:IPLab1LungAbscess3.jpg|This low-power photomicrograph of lung from this case demonstrates one of the abscesses (arrows). Note that the material inside the abscess has been | + | File:IPLab1LungAbscess3.jpg|This low-power photomicrograph of lung from this case demonstrates one of the abscesses (arrows). Note that the material inside the abscess has been degraded and removed. Note the loose necrotic material inside the abscess. This material is made up of inflammatory cells (primarily dead white blood cells) and necrotic lung tissue. |
| − | |||
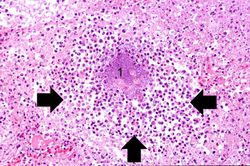
File:IPLab1LungAbscess5.jpg|This is a low-power photomicrograph of lung tissue containing a large abscess. The center of the abscess contains necrotic debris (1) and there is a rim of viable inflammatory cells (arrows) surrounding this abscess. | File:IPLab1LungAbscess5.jpg|This is a low-power photomicrograph of lung tissue containing a large abscess. The center of the abscess contains necrotic debris (1) and there is a rim of viable inflammatory cells (arrows) surrounding this abscess. | ||
File:IPLab1LungAbscess6.jpg|This high-power photomicrograph demonstrates a small abscess (arrow) with a necrotic center. | File:IPLab1LungAbscess6.jpg|This high-power photomicrograph demonstrates a small abscess (arrow) with a necrotic center. | ||
| − | File: | + | File:IPLab1LungAbscess8.jpg|This high-power photomicrograph shows the center of this abscess which contains inflammatory cells (primarily neutrophils) (arrows). There is a bacterial colony in the center of this abscess (1). |
| − | |||
</gallery> | </gallery> | ||
Latest revision as of 18:23, 1 August 2019
Contents
Clinical SummaryEdit
This 67-year-old male with advanced colon cancer underwent palliative surgery to remove a bowel obstruction. During the surgery the patient had several episodes of hypotension and after surgery he required ventilator support. Four days later the patient developed a fever and his white blood cell count was 15,256 cells/mm3. A chest x-ray demonstrated infiltrates in both lungs, which worsened over the next several days. His overall condition continued to deteriorate and he died 12 days after surgery. At autopsy, the lungs were markedly consolidated and had several focal abscesses that were 2 to 4 cm in diameter. Liquefied material poured out from these abscesses when the lungs were sliced.
ImagesEdit
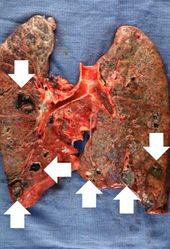
This is a gross photograph of the lungs from this case. Note the abscesses (arrows) especially in the lower lobes. The entire lung is consolidated.
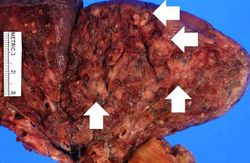
This is a closer view of the lung from this case. In this section of upper lobe there are multiple areas of early abscess formation (arrows). Note the circumscribed whitish-tan lesions. These lesions are filled with white blood cells.
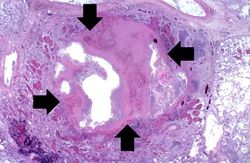
This low-power photomicrograph of lung from this case demonstrates one of the abscesses (arrows). Note that the material inside the abscess has been degraded and removed. Note the loose necrotic material inside the abscess. This material is made up of inflammatory cells (primarily dead white blood cells) and necrotic lung tissue.
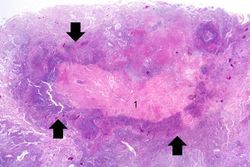
This is a low-power photomicrograph of lung tissue containing a large abscess. The center of the abscess contains necrotic debris (1) and there is a rim of viable inflammatory cells (arrows) surrounding this abscess.
This high-power photomicrograph demonstrates a small abscess (arrow) with a necrotic center.
This high-power photomicrograph shows the center of this abscess which contains inflammatory cells (primarily neutrophils) (arrows). There is a bacterial colony in the center of this abscess (1).






Virtual MicroscopyEdit
Study QuestionsEdit
Additional ResourcesEdit
ReferenceEdit
Journal ArticlesEdit
- Brandenburg JA et al. Clinical presentation, processes and outcomes of care for patients with Pneumococcal pneumonia. J Gen Intern Med 2000 September; 15(9): 638–646.
ImagesEdit
Related IPLab CasesEdit
Palliative surgery provides alleviation but is not curative.
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.
Consolidation is the filling of lung air spaces with exudate--this is a sign of pneumonia.
An abscess is a collection of pus (white blood cells) within a cavity formed by disintegrated tissue.
An abscess is a collection of pus (white blood cells) within a cavity formed by disintegrated tissue.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.